Today in 5-minute refresher lectures I will be discussing hepatitis B. Always follow your local guidelines and seek specialist advice. This lecture is only intended as a brief overview.
{youtube}ryh4QAmeBcM{/youtube}
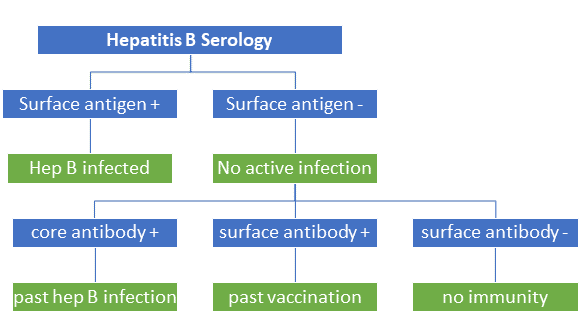
Hepatitis B is a virus that affects millions of people around the world. It is vertically transmitted during childbirth, with blood to blood contact as well as sexual transmission. When exposed as a child 90% develop chronic infection, whereas adult develop chronic infection in less than 10%. Interpreting serology is easy if you follow these simple steps. First determine if there is active infection with a positive surface antigen. Then determine if there was past infection due to the presence of the core antibody. Lastly check the surface antibody which becomes positive after vaccination.
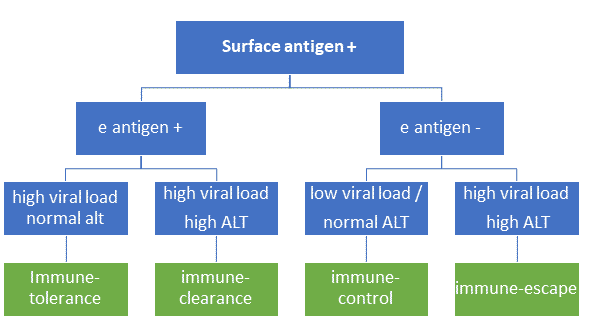
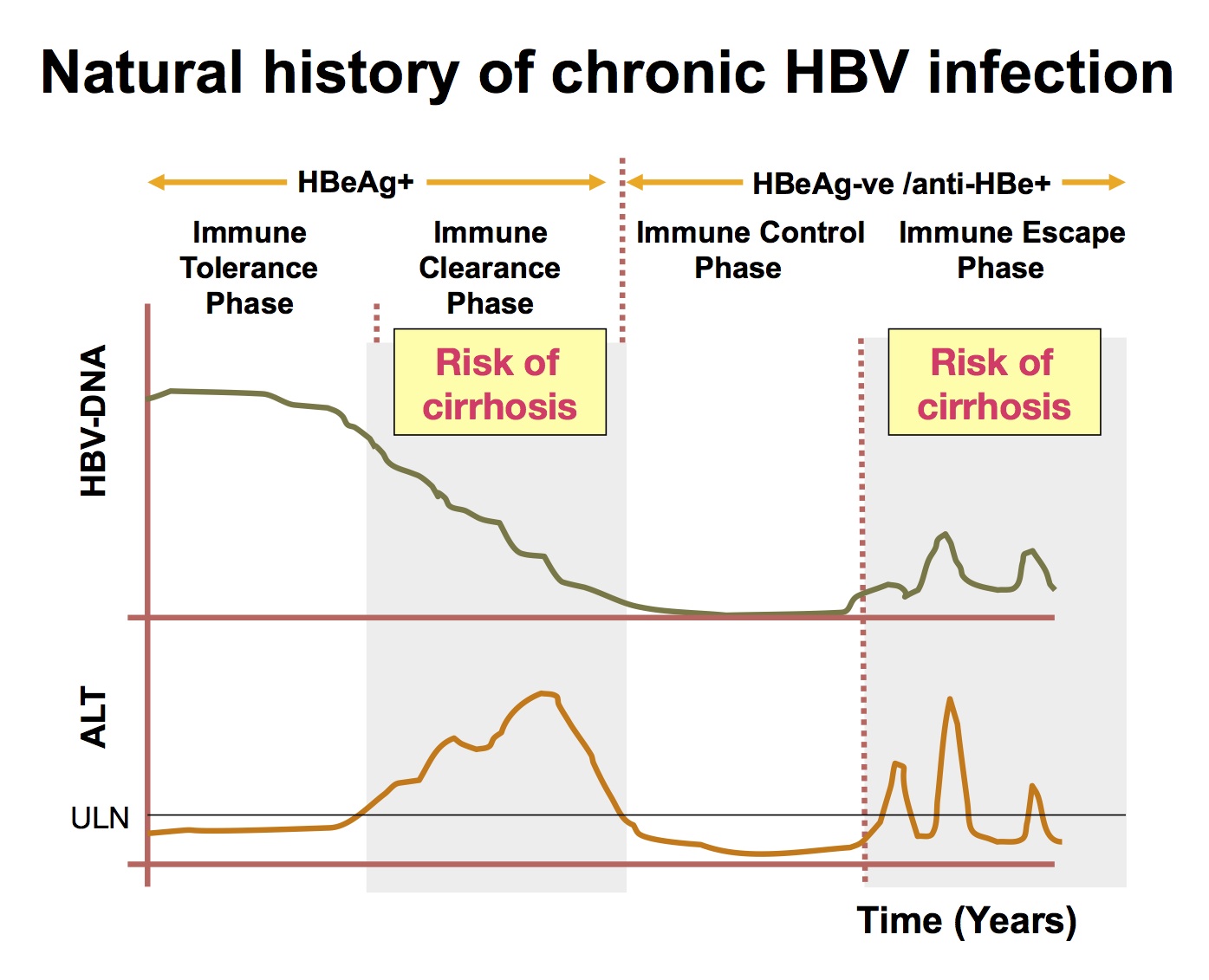
To determine the management, one must first understand the natural history of hepatitis B. In childhood there is a very high viral load, but the virus does not cause any liver inflammation with a normal ALT. Usually around a patient 2nd decade the patients immune system creates an extra antibody against the hepatitis E antigen, which causes liver inflammation with an elevated ALT due to the immune system attacking infected liver cells. With these extra e antibodies, the patient then goes into the immune control phase where these is low viral load and no liver inflammation with a normal ALT. However, the viral can develop a mutation in the promoter region of the e antigen gene. This stops production of e antigen by the virus and therefore allows it to escape the immune system. The immune escape phase is characterised by high ALT, high viral load, but negative e antigen.
Treatment of hepatitis B should be initiated by a gastroenterologist. In general, we treat people with antiviral treatment such as tenofovir or entecavir when people are in the immune-clearance or immune escape phase. We also treat people with cirrhosis regardless of viral load. A Chinese study randomised pregnant women to placebo vs tenofovir and found that vertical transmission risk increased when viral load > 6 log 10. Pregnant women with high viral load should be started on tenofovir during 3rd trimester and continued for 6 months post-partum.
Some patient remain the immune-tolerance phase and we know that the risk of liver cancer has a linear relationship to the viral load. The special authority requirement has been removed in New Zealand for anti-viral treatment, allowing us to also treat these patients that are at higher risk for the development of cirrhosis and liver cancer.
I hope you enjoyed this brief overview of hepatitis B. In New Zealand there is the hepatitis foundation who offers a fantastic service to monitor hepatitis B patients with regular blood tests. Please consult a gastroenterologist for any specific patient questions.